Dès les premiers mois de vie, de nombreux parents sont confrontés au muguet buccal, une infection fréquente chez les bébés. Bien que bénin, ce trouble peut perturber l’alimentation et l’humeur de votre enfant, ce qui peut être source d’anxiété. Le système immunitaire encore en développement chez les nourrissons les rend plus vulnérables à ce type d’infection, notamment après l’accouchement ou lors de traitements antibiotiques. Comprendre les causes du muguet et savoir comment agir peut considérablement apaiser vos inquiétudes et assurer le confort de votre bébé.
Qu’est-ce que le muguet buccal ?
Le muguet buccal, aussi appelé candidose buccale, est une infection courante chez les nourrissons, souvent source d’inquiétude pour les parents. Ce terme désigne une prolifération de Candida albicans, une levure naturellement présente dans le corps. Chez un bébé, le système immunitaire encore immature permet parfois à cette levure de se développer de manière excessive, provoquant des plaques blanches dans la bouche. Ce n’est pas grave en soi, mais cela peut être inconfortable pour votre enfant, surtout lors des tétées ou des repas.
Pourquoi mon bébé a-t-il du muguet ?
Plusieurs facteurs peuvent favoriser l’apparition du muguet. Parmi les plus courants, on trouve l’accouchement par voie basse, durant lequel le champignon peut être transmis de la mère à l’enfant. Les bébés prématurés ou ceux ayant reçu des antibiotiques récemment sont aussi plus à risque, car ces traitements peuvent perturber l’équilibre des bonnes bactéries. L’utilisation de tétines, de biberons ou une hygiène buccale insuffisante peuvent également contribuer à son apparition.
Vous allaitez ? Sachez que le muguet peut aussi se transmettre entre l’enfant et la mère, rendant l’allaitement douloureux. Les mamelons peuvent être rouges, sensibles et montrer des signes de desquamation (la peau semble partir en petits lambeaux par endroits). Si vous ressentez une gêne inhabituelle pendant la tétée, il est important d’en parler à votre médecin ou à un conseiller en lactation.


Les symptômes du muguet chez bébé
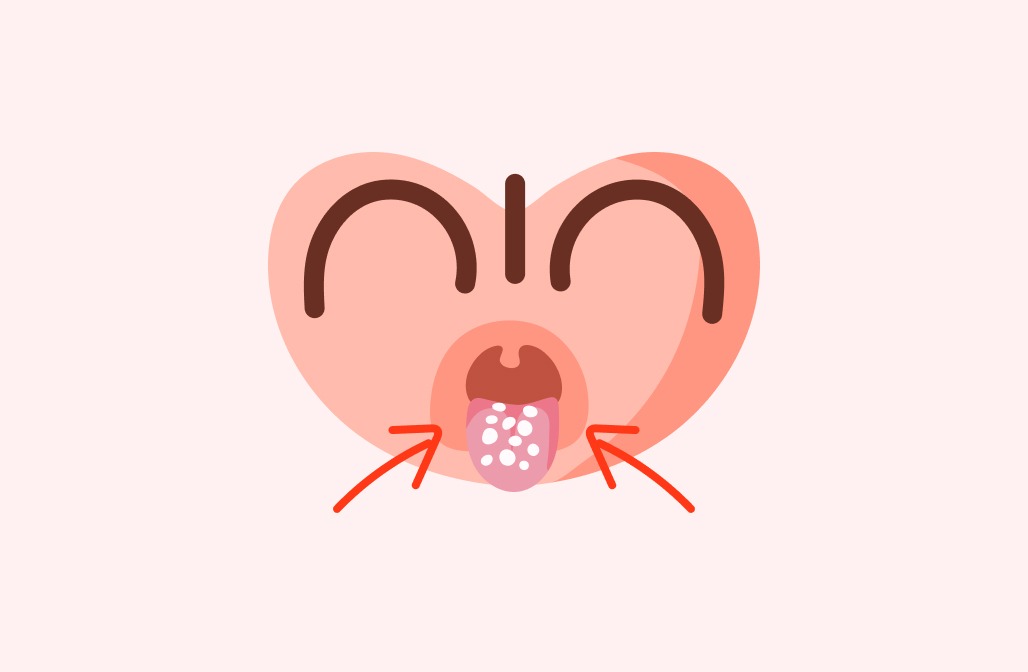
Les signes les plus évidents sont des plaques blanchâtres dans la bouche de votre bébé : sur la langue, l’intérieur des joues ou le palais. Ces plaques ressemblent à du lait caillé mais ne disparaissent pas facilement au frottement. Vous pouvez remarquer que votre bébé devient plus irritable, refuse de manger ou semble avoir du mal à téter. En plus de la bouche, le muguet peut parfois être associé à un érythème fessier, causé par la même levure qui se développe dans un environnement humide.
Vous vous demandez peut-être : « Est-ce vraiment du muguet ou juste des résidus de lait ? ». Une astuce simple consiste à nettoyer doucement la langue avec une compresse stérile imbibée d’eau. Si les taches ne partent pas, il s’agit probablement de muguet.
Quel est le traitement du muguet chez le bébé ?
La bonne nouvelle, c’est que dans la plupart des cas, le muguet est bénin et se traite facilement. Voici quelques soins pratiques pour aider votre bébé à guérir rapidement :
Traitements naturels à domicile
- Nettoyer les lésions : Utilisez une compresse imbibée d’eau bicarbonatée pour nettoyer délicatement la bouche de votre bébé, surtout avant les repas. Cela peut aider à réduire la prolifération de la levure.
- Changer et stériliser les sucettes et tétines régulièrement. Assurez-vous que tout ce qui entre en contact avec la bouche de votre bébé soit propre.
- Hygiène des mains : Lavez-vous soigneusement les mains avant de toucher la bouche de votre bébé, surtout après avoir changé ses couches.
Traitement médical : consulter un médecin
Si les plaques persistent ou si votre bébé semble particulièrement gêné, un traitement antifongique, souvent sous forme de gel ou de gouttes, pourra être prescrit par votre médecin. Les médicaments comme la nystatine ou le miconazole sont couramment utilisés et doivent être appliqués directement sur les zones touchées plusieurs fois par jour.
Prévenir le muguet chez le nourrisson : conseils pratiques
Pour prévenir le muguet, une hygiène rigoureuse est essentielle. Voici quelques mesures simples pour minimiser les risques :
- Maintenir une bonne hygiène buccale : Nettoyez délicatement la bouche de votre bébé après chaque repas, surtout s’il est allaité ou boit au biberon.
- Stérilisez les accessoires d’allaitement : Que ce soit les tétines, les sucettes ou les biberons, une stérilisation régulière est nécessaire pour éviter la prolifération de Candida.
- Soins des mamelons : Pour les mères allaitantes, laver et sécher soigneusement les mamelons après chaque tétée peut réduire le risque de transmission.
Les questions des parents
Comment différencier le muguet des résidus de lait ?
Pour différencier le muguet des simples résidus de lait, il est conseillé d’utiliser une compresse stérile imbibée d’eau pour nettoyer doucement les zones touchées. Si les taches blanches restent en place et ne se détachent pas facilement, il est probable que votre bébé souffre de muguet.
Le muguet est-il douloureux pour le bébé ?
Le muguet peut être inconfortable, surtout lorsqu’il affecte l’alimentation. Votre bébé peut pleurer plus souvent, refuser de téter ou montrer des signes d’irritabilité. Cela peut rendre les moments de repas plus difficiles, mais heureusement, il existe des solutions simples pour soulager votre enfant.
Peut-on prévenir le muguet avec une alimentation spécifique ?
Il n’existe pas de régime spécifique pour prévenir le muguet, mais maintenir une bonne hygiène buccale et éviter l’excès d’antibiotiques quand ce n’est pas nécessaire peuvent aider. Les probiotiques et une alimentation équilibrée pour la maman peuvent aussi favoriser un microbiote sain, ce qui peut indirectement contribuer à la prévention.
Quels sont les signes de muguet chez une mère allaitante ?
Chez les mamans allaitantes, le muguet se manifeste souvent par des mamelons douloureux, rouges ou sensibles, avec parfois des crevasses. Vous pouvez aussi ressentir des douleurs inhabituelles pendant la tétée. Ces symptômes doivent être pris au sérieux et il est conseillé de consulter un professionnel de santé pour un traitement approprié.
Combien de temps dure le traitement du muguet ?
Le traitement du muguet dure généralement entre 10 et 14 jours, selon les recommandations de votre médecin. Il est important de suivre ses indications pour l’application des antifongiques et de persister jusqu’à la fin du traitement pour éviter toute récidive.
Le muguet chez le bébé est une affection fréquente et généralement sans gravité. Avec quelques précautions et un suivi attentif, votre bébé se remettra rapidement. N’oubliez pas de toujours observer les réactions de votre enfant et n’hésitez pas à demander conseil à un professionnel de santé si vous avez des doutes. Votre vigilance et votre amour sont les meilleurs alliés de la santé de votre bébé !
Pour aller plus loin :